

Female Urinary Incontinence
Incontinence is a term used to describe the involuntary loss of urine. Urine is made in the kidneys. The kidneys, which sit high in the back under the rib cage, filter the blood and extract excess waste products and fluid to form the urine. Once made in the kidneys, the urine travels down a tube on each side called the ureter until it reaches the bladder.
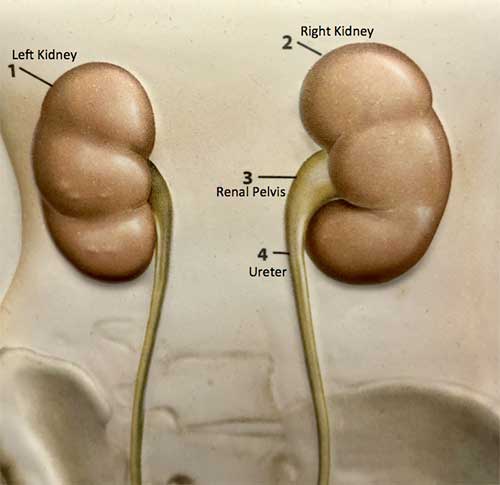
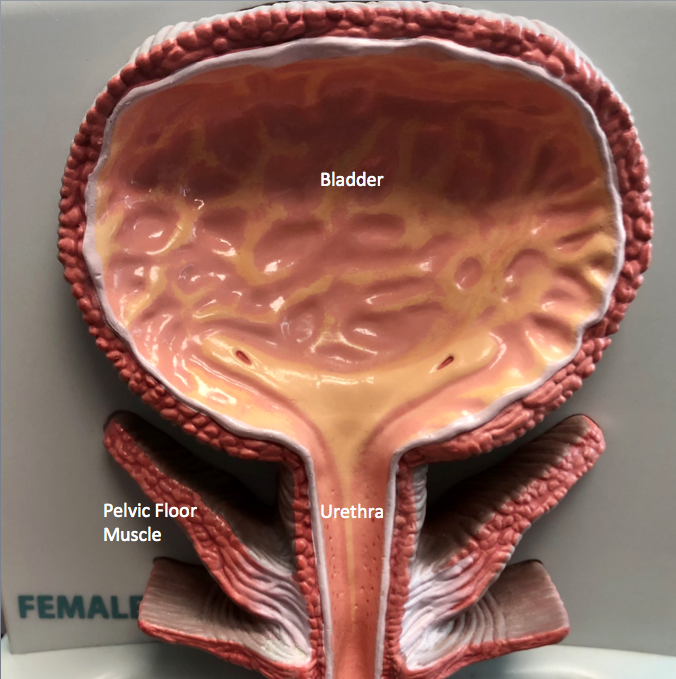
The bladder’s job is to store the urine until it is full and then it empties urine to the outside through the urethra.
Incontinence occurs when the bladder doesn’t store the urine properly. In general, there are two common types of incontinence – stress incontinence and urge incontinence. Stress incontinence occurs when there is a sudden stress to the bladder, (e.g. coughing, sneezing, running, dancing, changing from sitting to standing) that causes urine to leak from the bladder through the urethra. This type of incontinence is usually not preceded by a sense of the need to urinate. Urge incontinence occurs when one senses the urge to urinate, but before she can reach the bathroom urine begins to come out on its own. There are other less common types of incontinence as well.
Stress Incontinence
Stress incontinence usually occurs as a result of weakening of the support structures in the pelvis that hold up the bladder and urethra. Childbirth and menopause are two factors that may increase a woman’s chance of developing stress incontinence.
During the examination for symptoms of incontinence the abdomen and groin areas are inspected. The position of the bladder and urethra are checked. An internal exam may be done to make sure that there is not anything pressing on the bladder and urethra. Sometimes in addition to the office examination, a urodynamic study may be recommended. During this study the capacity of the bladder and the pressure at which urinary leakage takes place can be measured precisely. A small catheter is inserted into the bladder and then the bladder is filled to evaluate its storage ability and to identify when leakage takes place.
We usually manage stress incontinence with a stepwise approach. Kegel exercises are usually tried as part of the initial management. These are done by squeezing the muscles of the pelvis for 5-10 seconds at a time for 30-40 times a day. One way to remember to do the exercises frequently enough is to squeeze the muscles each time you hear a commercial on the radio or see an ad on T.V. To learn how to squeeze the “right” muscles in the pelvis, contract the pelvic muscle during urination that makes the flow of urine stop. Once you figure out which muscle stops urination that is the one to “exercise”. After learning which muscle you need to squeeze, do not continue to do this during urination on a regular basis. Rather do it 30-40 times during the day when not urinating (i.e. riding in a car, sitting in a chair, standing in a store).
Learn How to Do a Proper Kegel Exercise
Watch Dr. Tran explain how to do a proper Kegel exercise:
Kegel exercises lessen stress incontinence in about half of patients, but the effect may not be noticeable until after 3-4 months of carrying out these exercises. Some other methods occasionally used to help with stress incontinence include vaginal Premarin cream and medicines to increase the tone of the urinary sphincter. Vaginal Premarin cream may improve the support of the bladder and urethra. Some of the drugs that can increase the strength of the urinary sphincter include Entex LA, Sudafed and Ornade.
If the above methods are unsuccessful and when the symptoms are troublesome enough that a patient wants something done, surgical re-suspension of the bladder and urethra can be carried out. Urethral slings are now the standard of care with 85-95% success rates typically. Complications of surgery can include bleeding and infection, in addition to the other general risks of surgery.
For some women with stress incontinence, the bladder and urethra are in the proper place but problems develop due to failure of the urethra to close tightly. In this case, collagen may be injected underneath the surface of the urethra to create a better seal. This technique is carried out on an outpatient basis with minimal sedation. As many as 75% of women notice a favorable improvement. Some women require re- treatment within several years if the collagen becomes reabsorbed.
Urge incontinence occurs when the bladder involuntarily contracts and begins to empty urine. If the bladder had its way, it would contract all the time and never fill with urine. Normally, the bladder is prevented from contracting involuntarily by a reflex. When the reflex doesn’t work properly, the bladder has an “uninhibited contraction” and may go on its own. In this circumstance a patient may feel the urge to void, but before she can reach the bathroom, the urine is already coming out. A common scenario people describe is that when they reach the door of their house, they feel an intense need to go. Before they can get the door unlocked and get into the bathroom, they begin to get wet.
Medications are used to manage urge incontinence. These pills, such as Levbid, Detrol, Ditropan, and Urised suppress “uninhibited bladder contractions” and lessen the likelihood of the bladder going on its own.
Many times a patient has a mix of both stress and urge incontinence and a combination of the above treatments may be used. Incontinence is a common problem that affects many women. With appropriate evaluation and treatment many women can be helped.
Additional Information
Bladder Satisfaction Survey
Urinary History
Pelvic Floor Therapy for Women
Estrogen Cream Application
Estrogen Cream in Women with Pelvic Floor Disorders
Seat Cushion
Contact us to request an appointment or ask a question. We're here for you.