

Renal Cysts
The urinary tract begins with the kidneys. The kidneys, one on each side, sit high in the upper abdomen partially underneath the rib cage.
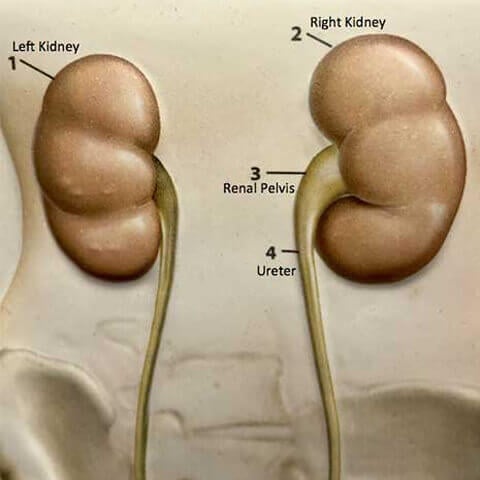
They filter the blood to extract excess waste products and fluid to form the urine. Urine, once formed in the kidneys, travels through a tube on each side, called the ureter, down to the bladder. Urine is constantly being made by the kidneys and being transported through the ureters into the bladder. The bladder stores urine until full and then empties to the outside through the urethra. The urinary system is the same in both men and women from the level of the kidneys to the bladder. In men, the prostate, which is a gland that is part of the reproductive system, encircles the first part of the urethra.
A variety of disorders may affect the kidney which can include stone, obstruction, mass (solid growth), or cyst. Renal cysts are common, and more than one third of all people over age 50 have cysts in the kidney. Renal cysts are often detected during an imaging study (ultrasound or CT scan) carried out to investigate some other problem. A cyst is a thin fluid-filled structure that originates from the surface of the kidney. There may be a single cyst or there may be multiple cysts present. Cysts typically do not cause any type of symptoms, and usually do not cause problems with compression of adjacent organs (other structures next to the kidney, such as the liver or intestine). Cysts usually do not interfere with kidney function.
When cysts are present, they are further characterized by their appearance on the imaging studies (see Table 1). In broad terms, cysts can be divided into categories of simple cysts versus complex cysts. Simple cysts have thin walls with no evidence of wall thickening or internal walls. Complex cysts may be thick-walled or have areas of calcification or nodular change. In addition, a complex cyst may have multiple walls (called septation).
Simple cysts do not need any intervention or further follow up. Complex cysts, however, do need further attention.
Complex cysts pose a concern because a subset of complex cysts may have cancerous growth. Of note, most cancerous growths in the kidney are solid, not cystic. Yet some cancers of the kidney may have a cystic component. Strategies are available to predict whether a complex cyst may be associated with cancerous change.
The approach to cysts depends on the cyst characteristics. Bosniak I-II cysts do not require any further imaging or follow up. Bosinak II F cysts have multiple septae. The septa or cysts wall may contain calcification or be thickened. There is a risk of cancer so follow up imaging is required (“F” stands for “Follow”). These cysts are typically followed with ongoing imaging studies at 6-12 month intervals. Bosniak III cysts have irregular walls (or septa), coarse calcification, or some degree of variable appearance. The risk of cancer in this type of cyst may be 50%. Bosniak category IV cysts have definite nodular change and areas that enhance when dye is giving during a CT scan.
Bosniak III-IV cysts are most likely associated with cancerous change and should be addressed through surgical intervention.
When intervention is necessary, surgical choices include thermal ablation (freezing or burning), removing the cyst or complete removal of the kidney. Cyst excision is typically carried out through laparoscopy or robotic surgery. A fiber optic camera is placed through a “port” (small 1 cm incision) in the abdomen. Instruments are passed through other ports which allow the surgeon to excise and remove the cyst.
Cysts in the kidneys are a common finding. The approach to cyst depends on the characteristics of the cyst noted on the imaging study. With appropriate urologic care, consisting of either serial follow-up or intervention, these disorders can be addressed effectively.
Bosniak Classification of Complex Renal Cysts
| Type | Description | Recommended Management | Risk of Cancer |
|---|---|---|---|
| I | Simple benign cyst. No calcifications, septa or solid components. No enhancement. | No follow-up necessary | Extremely low |
| II | Benign cyst that contains hairline septa. Short, thin areas of calcifications may be present. Septa and wall do not enhance. Hounsfield units <10. | No follow-up necessary | Very low |
| II F | Thickened cyst wall, multiple septae that may be thickened or contain calcium, Hounsfield units of 10-15, no significant enhancement with contrast. | Follow-up imaging | 3-10% |
| III | Cystic mass with thickened wall, thick irregular septum, cyst wall or septa enhance with contrast, Hounsfield units >15. | Surgery | 50% |
| IV | Cystic mass with thickened wall, thick irregular septum, cyst wall or septa enhance with contrast, Hounsfield units >15. | Surgery | 75-90% |
Cyst Decortication
Are Cysts on the Kidneys Serious?
Contact us to request an appointment or ask a question. We're here for you.