19415 Deerfield Avenue • Suite 112 • Lansdowne, VA 20176 • 703-724-1195
1860 Town Center Drive • Suites 150 & 160 • Reston, VA 20190 • 703-480-0220
224-D Cornwall Street, N.W. • Suite 400 • Leesburg, VA 20176 • 703-443-6733
24440 Stone Springs Blvd • Suite 545 • Dulles, VA 20166 • 703-957-1022
1801 Robert Fulton Drive • Suite 510 • Reston, VA 20191 • 703-783-5355
Bladder Cancer
Bladder cancer is a common condition treated by urologists. It is estimated that approximately 70,000 Americans are diagnosed with bladder cancer each year. Male patients outnumber female patients three to one, making bladder cancer the fourth most common cancer in men. The key to success is careful, regular follow-up to identify disease at a superficial stage in an effort to prevent progression to disease invading into the bladder wall. Learn about Bladder Cancer at The Urology Group: Urological Cancer Center.
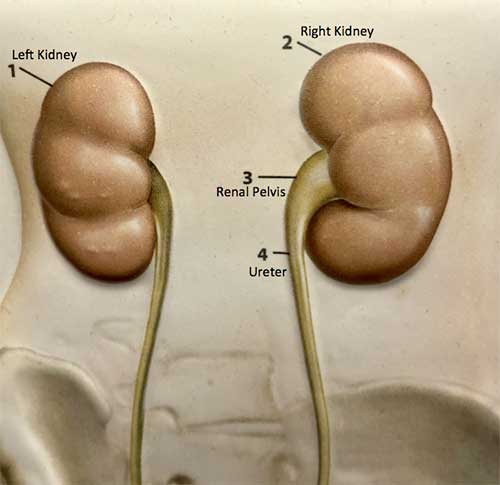
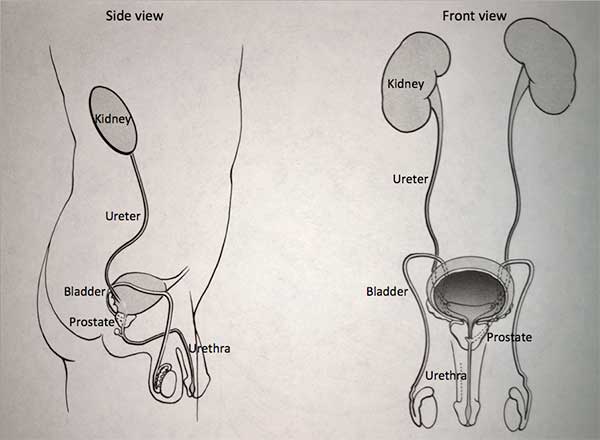
The bladder is part of the urinary system. The function of the urinary system is to clear waste products from the blood. The urinary tract consists of the kidneys, ureters, bladder and the urethra. The urinary tract begins with the kidneys. The kidneys, one on each side, sit high in the upper abdomen partially underneath the rib cage.
They filter the blood to extract excess waste products and fluid to form the urine. Once the urine is made by the kidneys it is transported down through tubes called the ureters to the bladder. The bladder sits in the pelvis, which is the area in the lower abdomen. The bladder stores urine until full then empties the urine to the outside through the urethra. The urinary system is the same in both men and women from the level of the kidneys to the bladder. In men, the urethra is longer and is encircled by the prostate, which is a gland that is part of the reproductive system.
Urination occurs when the urinary sphincter muscle relaxes and the bladder muscle contracts to expel the urine. The bladder consists of three layers. The inner lining layer of the bladder, called the mucosa, is formed by a type of cell called transitional cell. The next layer, the lamina propria, provides support to the mucosa. The third layer is the bladder muscle itself. Most types of bladder cancer are transitional cell cancers, which means they arise from the transitional cells in the inner lining layer of the bladder.
It is not always clear what causes bladder cancer to form. Cigarette smoking and exposure to industrial chemicals are clearly defined risk factors. Cigarette smoking alone has been estimated to cause 50% of all bladder cancers. Workplace exposure to chemical compounds such as paints and solvents may cause another 20-25% of bladder cancer cases.
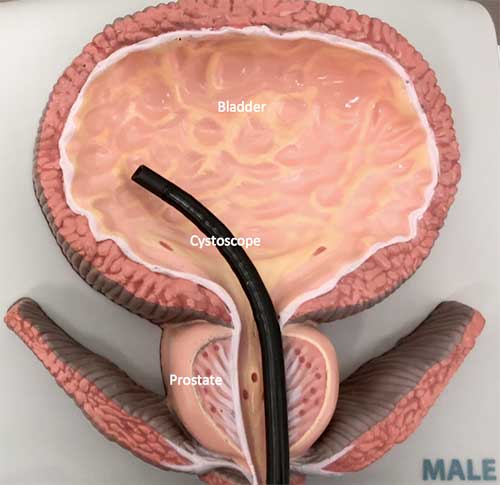
Bladder cancer often first shows up as blood in the urine. This may occur as gross hematuria (visible blood which can be seen in the urine) or microscopic hematuria (blood which can be seen only on a urinalysis test done in a doctor’s office). The presence of blood in the urine itself does not signify bladder cancer. There are many different potential causes for blood in the urine. Bladder cancer may also cause urinary symptoms including dysuria (pain with urination), frequency (the need to void more often than usual), and urgency (a sense of the need to urinate immediately). At times, bladder cancer may be discovered incidentally during an inspection of the bladder for some other reason. Bladder cancer is typically diagnosed by a cystoscopy. Cystoscopy is the inspection of the lining of the bladder with a fiberoptic catheter. It may also be identified with the use of cytology, in which a test like a “Pap smear” is done on the cells shed during urination. At times, a bladder tumor may be identified on x- rays of the urinary system, including studies such as an IVP, ultrasound or CT scan.
When an abnormality is identified, the next step is cystoscopic removal of the bladder tumor or a biopsy of an abnormal appearing area. Cystoscopic removal of a bladder tumor (also known as transurethral resection of bladder tumor or TURBT) is done in the operating room under anesthesia. Biopsies of the bladder can be carried out at the same time. These types of procedures are done through the cystoscope, the fiberoptic instrument placed through the urethra. It is not necessary to make an incision.
At times, these procedures are carried out as an outpatient. Other times, overnight hospitalization may be required. In some cases, a catheter (a tube in the urethra to drain urine from the bladder) may be left indwelling for a period of time.
Improving the Detection of Bladder Cancer
Reston Hospital Center has performed its first blue light cystoscopy procedure – a new technology used to detect non-muscle invasive bladder cancer. Learn more, read the press release here.
We are the first practice in Virginia to offer rigid Blue Light cystoscopy:
This technology allows enhanced visualization of tumors in the operating room such that we can see and remove suspicious areas in the same operative setting.
Blue Light Cystoscopy has been shown to increase detection of bladder cancer by 20%. Blue Light Cystoscopy has been shown to increase detection of a cancerous change called “carcinoma in situ” by 35%. Carcinoma in situ is a flat lesion that is difficult to appreciate with standard white light cystoscopy.
Table 1:
Staging of primary bladder cancer tumors (T)
Ta
Noninvasive papillary tumor (confined to urothelium)
Tis
CIS Carcinoma (high grade “flat tumor” con- fined to urothelium)
Ta
Noninvasive papillary tumor (confined to urothelium)
Tis
CIS Carcinoma (high grade “flat tumor” con- fined to urothelium)
Once the bladder tumor is removed, further information is available from the pathology report about the type of cancer. When evaluating cancer, the concepts of grade and stage are important. Grade refers to the appearance of the cells under a microscope. Typically there are three grades: low (I), intermediate (II) and high (III). The grade indicates the biologic potential of the tumor. Low-grade tumors tend to be less aggressive. Stage describes the depth of penetration of the bladder cancer into the bladder wall.
The most commonly used system is the TNM system. The T level refers to the depth of invasion into the bladder wall as shown in table 1.
Almost 90% of cases of transitional cell cancer of the urinary bladder are superficial (stage Ta, Tis,T1). These can be treated with cystoscopic removal. In some patients, it can be predicted that they are likely to have recurrent disease. Whatever it was that first caused the cells in the bladder to form a tumor has affected the remainder of the cells in the bladder, so that new tumors can form at some point in the future. For that reason, regular cystoscopic surveillance is mandatory to monitor for recurrence. Cystoscopy is carried out at three-month intervals during the first two years, at six-month intervals for the next three years and yearly thereafter. Urinary cytology may be done in the same setting as well. In some patients with increased risk factors, an IVP may be carried out at selected intervals also.
For patients in whom the risk of recurrence is high, further treatment with intravesical therapy may be indicated. Intravesical means “within the bladder.” Therapeutic agents are placed directly into the bladder through a catheter. This treatment is carried out in the office. Intravesical agents commonly used are thiotepa, doxorubicin, mitomycin C and bacillus Calmette-Guerin, more commonly known as BCG. Thiotepa, doxorubicin and mitomycin are drugs, which act directly on the transitional cells. BCG is a vaccine used to stimulate the immune system to lessen the potential for new bladder tumors to develop. BCG is currently the most commonly used intravesical agent. Typically it is initially given once a week for a six week course, followed by a three week course at three and six months intervals after initial treatment. It is then given at additional six month intervals for a total of three years. Typical side effects after BCG treatment include: symptoms of cystitis (frequency, urgency, and dysuria), low-grade fever and flu-like symptoms. Blood may be present in the urine for one to two days after treatment. If high fever (greater than 101.5) develops, a physician should be notified. A separate information sheet is available describing instructions for BCG treatment.
For a small minority of patients, bladder cancer may involve the deeper bladder layers (stage T2-T4). In these patients, the primary treatment is cystectomy (surgical removal of the bladder) with urinary diversion. Urinary diversion choices include a conduit approach (directing the urine to a segment of intestine which comes out to the skin as a stoma so that the urine can be collected in a bag) or a continent diversion (a new bladder is created out of intestine). In patients who require cystectomy, chemotherapy may be required as well.
Bladder cancer is a common condition which urologists treat frequently. The key to success is careful, regular follow-up to identify disease at a superficial stage in an effort to prevent progression to disease invading into the bladder wall.
We are pleased to offer online appointment request! New patients can request a call to schedule an appointment. Established patients seen in the last 3 years can request an appointment with one of our nurse practitioners/physician assistants.