19415 Deerfield Avenue • Suite 112 • Lansdowne, VA 20176 • 703-724-1195
1860 Town Center Drive • Suites 150 & 160 • Reston, VA 20190 • 703-480-0220
224-D Cornwall Street, N.W. • Suite 400 • Leesburg, VA 20176 • 703-443-6733
24440 Stone Springs Blvd • Suite 545 • Dulles, VA 20166 • 703-957-1022
1801 Robert Fulton Drive • Suite 510 • Reston, VA 20191 • 703-783-5355
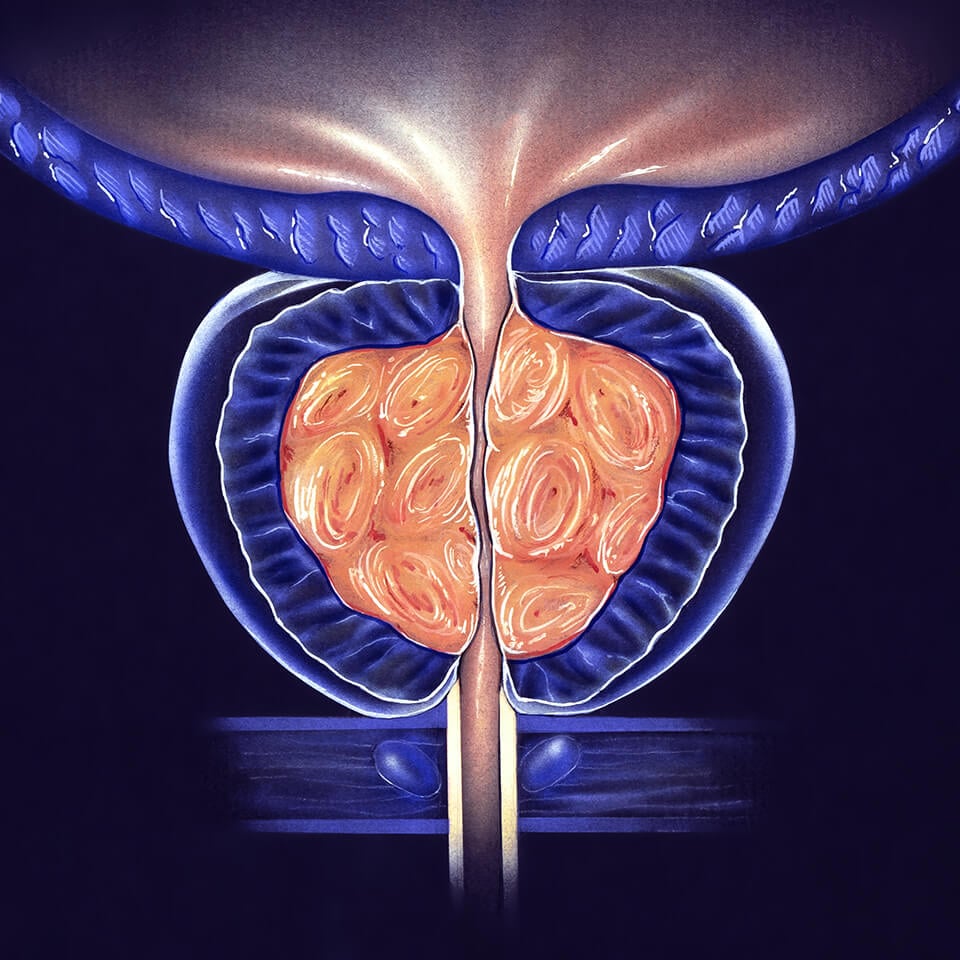
Benign Prostatic Hyperplasia (BPH)
Benign prostatic hyperplasia (BPH) refers to the normal enlargement of the prostate gland that occurs in men with aging. The prostate gland in adults remains a constant size until approximately age 40, when it begins to enlarge. Although BPH does not produce trouble in all men, 1 out of 4 men usually require treatment.
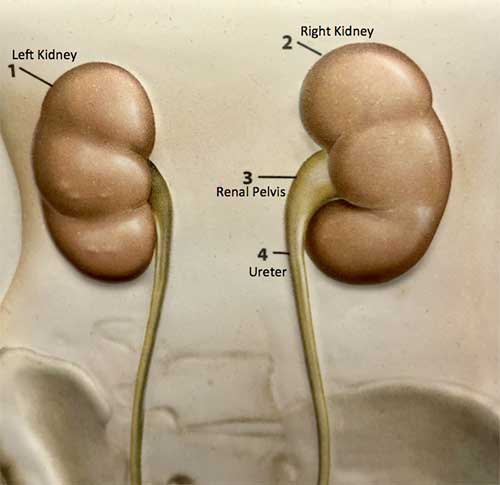
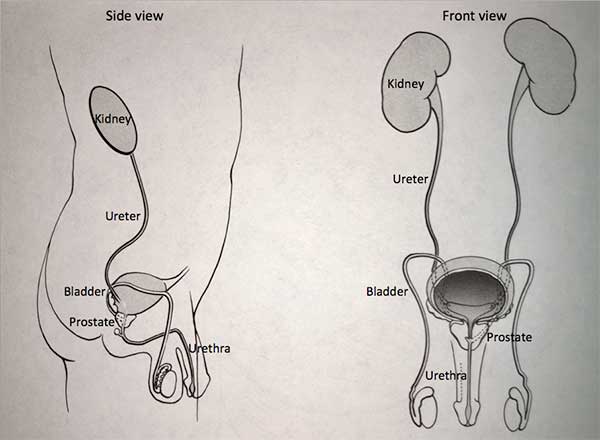
The urinary tract begins with the kidneys. The kidneys, one on each side, sit high in the upper abdomen partially underneath the rib cage.
They filter the blood to extract excess waste products and fluid to form the urine. Urine, once formed in the kidneys, travels through a tube on each side, the ureter, down to the bladder. Urine is constantly being made by the kidneys and transported through the ureters into the bladder. The bladder stores urine until full and then empties to the outside through the urethra. The prostate, which is a gland that is part of the reproductive system, forms the first part of the urethra.
What are the symptoms of prostate enlargement?
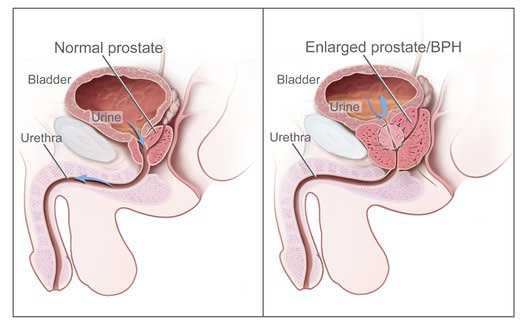
The enlarged prostate causes trouble when it restricts the flow of urine out of the bladder. As the prostate enlarges, it blocks the urinary pathway.
The bladder then has to work harder to overcome this increased resistance to urine flow. If the blockage is severe enough, the bladder may be unable to empty, leading to a condition called urinary retention. The onset of symptoms of BPH can be very gradual. Symptoms can include difficulty starting the flow of urine, decreased force of urination, and dribbling at the end of urination.
There may be incomplete emptying of the bladder which produces a sense of still feeling full even after attempting to pass the urine. Incomplete bladder emptying also leads to “double voiding” in which a man passes the urine and then has to urinate again within a period of 10 to 20 minutes.
Other symptoms include the need to pass urine more frequently than normal and the development of a sense of urgency, which is the need to pass the urine as soon as the urge is felt. One of the most common symptoms of BPH is being awakened from sleep to urinate.
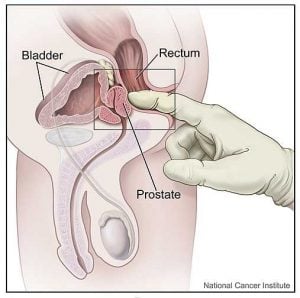
How is the prostate checked?
The diagnosis of BPH is made in a variety of ways. The most important is careful physical examination of the prostate by the physician. This is done by inserting a gloved finger into the rectum to palpate the surface of the prostate. A blood test to measure PSA, prostate specific antigen, is done to determine if prostate cancer may be present.
A bladder sonogram or scan is often done to check post void residual (the amount of urine left behind in the bladder after voiding). If residual urine is too high and is untreated, it may predispose the patient to kidney failure, infection or bladder stones. A urinary flow study may be done to measure the rate and force of urinary flow.
Does the enlarged prostate always need treatment?
There are a variety of ways to manage BPH. One of the most common is to “wait and watch.” If the symptoms are not particularly troublesome and if there is no impending danger of damage to the urinary tract, no intervention may be necessary. Often the symptoms progress only very gradually over time. Regular follow up exams at 6-12 month intervals are recommended.
When should the enlarged prostate be treated?
There are several indications for treatment of BPH. One of the foremost is urinary retention, which is the inability of the bladder to empty any urine. Intervention is also required when the enlarged prostate impairs drainage of urine out of the bladder and there is a large postvoid residual. This residual urine can block the drainage of the kidneys and lead to inadequate kidney function. (A bladder sonogram or scan may be done to make sure the residual is not too high). Severe bleeding or recurrent urinary tract infections are also symptoms which indicate the need for intervention. By far the most common indication for treatment is when difficulty with urination becomes so troublesome that the patient needs some relief.
What pills can be used for the enlarged prostate?
When intervention is necessary it may be possible to manage BPH with medication. There are two different types of medication that can be used. The first is called an alpha blocker and is designed to release the “grip” of the prostate as it crowds in on the urinary pathway.
The alpha blockers include Flomax (tamsulosin), Uroxatral (alfuzosin), Rapaflo (silodosin), Hytrin (terazosin), and Cardura (doxazosin). They reduce the compression of the urinary channel caused by the prostate. Many patients notice an immediate improvement in symptoms. Side effects can include low blood pressure, dizziness, tiredness and nasal congestion. Some men experience retrograde ejaculation, also known as dry climax. They have an orgasm but no fluid comes out (the semen backwashes into the bladder and is rinsed out with the next urination). Retrograde ejaculation does not cause any harm. Some men find retrograde ejaculation bothersome and they manage that issue by not taking their alpha blocker on the days they have sex. Alpha blockers may cause a condition known as intraoperative floppy iris syndrome which may cause operative complications in some men who have cataract surgery. Men with planned cataract surgery should avoid the initiation of alpha-blockers until their cataract surgery is completed.
The second type of medicine used to treat the enlarged prostate is designed to reduce the size of the prostate. Proscar (finasteride) and Avodart (dutasteride) are 5-Alpha-reductase Inhibitors (5-ARIs) which are taken daily on an ongoing basis. They can prevent progression of voiding bother due to BPH, reduce the risk of urinary retention and may lessen the need for future prostate-related surgery. Side effects are primarily sexually related and include decreased libido, ejaculatory changes, and ED. A small subset of men may get breast enlargement or tenderness. These effects are usually reversible and uncommon after the first year of therapy. Treatment with Proscar or Avodart is most useful in men with very large prostates, and it may take 6 to 12 months of treatments until results are noticed.
At times, the combination of both an alpha-blocker and a 5-ARI is an appropriate and effective treatment for patients with voiding bother associated with prostate enlargement.
What if pills do not work?
If patients do not respond to treatments with pills, then we consider a procedure or surgery.
Prostate Artery Embolization – procedure with our radiologist to plug the blood vessels to the prostate to make the prostate shrink.
UroLift – minimally invasive procedure that uses tiny implants to pull apart the enlarged prostate lobes and widen the urinary channel.
Rezum - minimally invasive procedure where steam vapor is injected into the prostate which kills prostate cells to shrink the prostate.
Aquablation –uses a water jet and robotic arm to remove excess prostate tissue.
Simple prostatectomy – a surgery, usually performed as a minimally invasive procedure with robotic assistance, to remove the part of the prostate that causes urinary blockage. Typically reserved for very large prostates.
We are pleased to offer online appointment request! New patients can request a call to schedule an appointment. Established patients seen in the last 3 years can request an appointment with one of our nurse practitioners/physician assistants.