
Prostate Cancer Radical Prostatectomy
Prostate cancer is one of the most common cancers to occur in men. Current estimates suggest that one in 10 men will develop prostate cancer.
How is prostate cancer diagnosed? What are treatment options?
Prostate cancer is usually diagnosed by trans rectal ultrasound and needle biopsy of the prostate. The widespread use of PSA testing in the United States has led to the diagnosis of prostate cancer at an earlier stage, which has led to improvement in long-term outcome. When prostate cancer is localized to the prostate, (known as stages T1-T2), it can be effectively treated with therapy directed to the prostate itself. Current choices for the management of localized prostate cancer include radical retropubic prostatectomy, external beam radiotherapy, and interstitial brachytherapy (or seed implant).
When cancer is diagnosed, the next step is to decide if staging studies need to be carried out. Staging studies can include bone scan, CT scan of the pelvis, and chest x-ray. The decision to carry out these studies depends on several factors, which include the PSA level, the Gleason score, and the number of positive biopsies.
Radical prostatectomy remains one of the principal therapies for early prostate cancer. It provides superior long-term outcome, and likely provides the best chance for a man to remain free of disease 15- 20 years after his diagnosis and treatment.
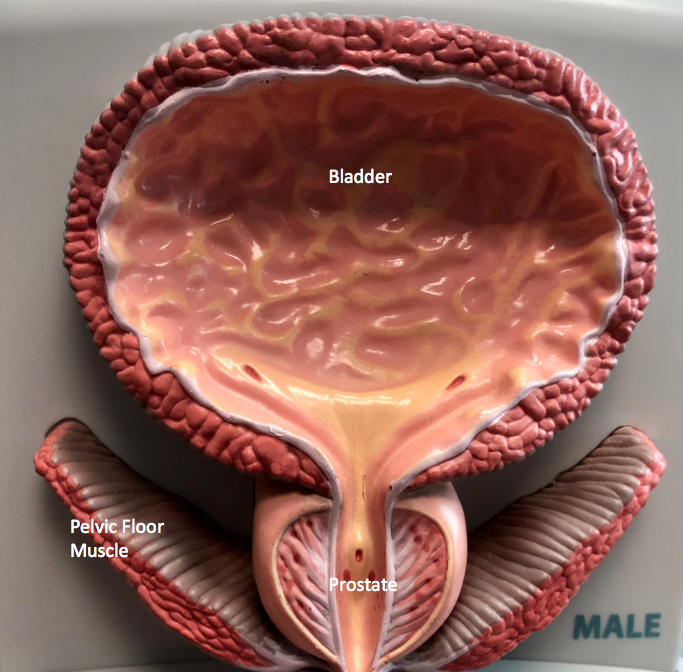
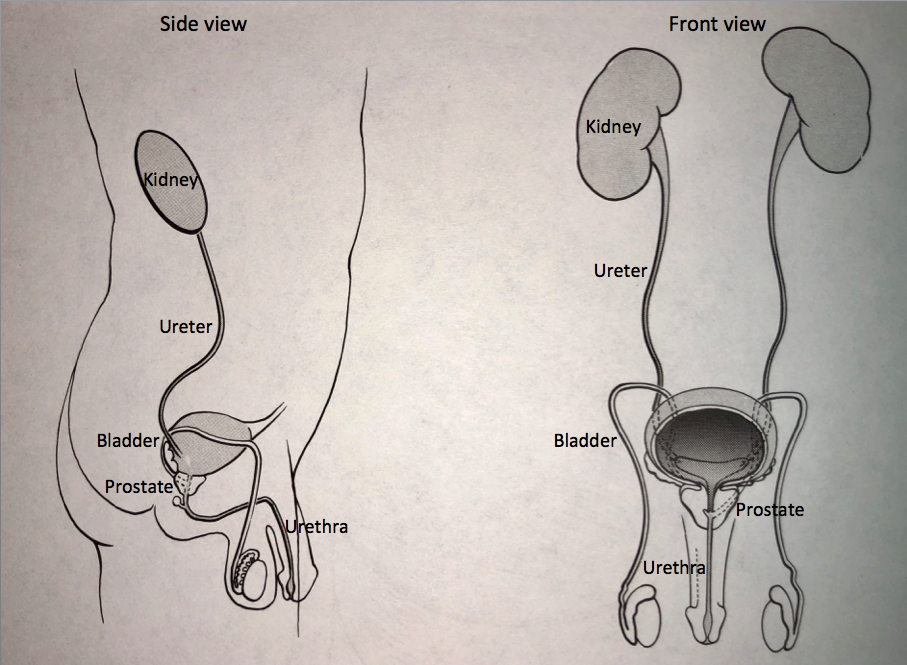
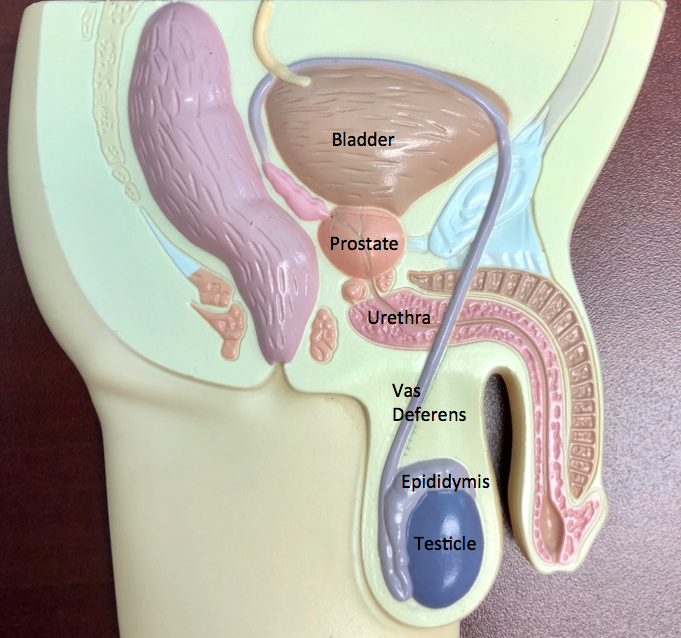
How is the urinary system put together? Where is the prostate?
The urinary system begins with the kidneys, which sit high in the upper abdomen. They make urine, which is transported through tubes called the ureters to the bladder, which holds urine until full. Once full, the bladder empties to the outside through the urethra, which is the urinary channel that runs through the penis. The prostate, which is a gland that is part of the reproductive system, forms the first part of the urethra just below the bladder. When urination takes place, the bladder contracts while the urinary sphincter relaxes so that the urine can be pushed from the bladder through the urethra to the outside.
What is role of radical prostatectomy? How is it done?
Radical prostatectomy is one of the principal treatments for early prostate cancer. It provides superior long-term outcome, and likely provides the best chance for a man to remain free of disease 15- 20 years after his diagnosis and treatment.
Radical prostatectomy refers to the surgical removal of the prostate and the attached accessory glands called the seminal vesicles. In the first part of the surgery, the lymph nodes adjacent to the prostate may be sampled to determine if there are areas of microscopic spread. Biopsy of the lymph nodes may help provide information with respect to long-term outcome. The prostate and seminal vesicles are then removed. The vas deferens, the tubes that carry sperm from the testicles to the prostate, are divided. The bladder is then rejoined to the urethra. A catheter, which is a tube to drain urine from the bladder, is placed. The catheter tube exits from the tip of the penis and is connected to a drainage bag. A surgical drain is placed next to the incision to drain fluid from the surgical site.
What is the da Vinci procedure?
There are two surgical approaches currently used. For years, radical prostatectomy has been done via an “open” approach. A lower midline abdominal incision is made from the belly button to the pubic bone. More recently, robot assisted da Vinci laparoscopic radical prostatectomy is widely used. The same surgery can be performed through a small incision using a fiber-optic camera.
The decision about using an open versus a laparoscopic technique depends on a patient’s overall health, body size, and the features of the prostate cancer. Both types of surgery typically take several hours.
What is the recovery after surgery?
Men are usually admitted to the hospital on the day of surgery, and discharged home after 1 or 2 days if all goes well. The surgical drainage tube is usually removed at the first or second day after surgery. Men are ready for discharge when they are able to keep liquids down, pills control their pain, and they are able to move around adequately on their own. Men are sent home with the catheter in, which typically remains in place for 7-14 days after surgery. The catheter is attached to a leg bag so that men are able to carry out their normal activities. A detailed postoperative instruction sheet describes the postoperative care. In short, once men are at home they are able to shower, take what they want to eat or drink, go up and down stairs, and move around as comfortable. Restrictions include no heavy lifting for six weeks. Men may be out of work anywhere from 2 to 6 weeks.
What are the risks of surgery?
Risks of radical prostatectomy are the same as those risks for any surgery procedure. These risks occur infrequently but can include heart irregularity, lung problems, blood clot in the leg, or infection. Antibiotics are given preoperatively to reduce the risk of infection. Special devices called venous compression stockings are used to reduce the risk of blood clots in the leg. Men are asked to avoid using aspirin, Motrin, or similar type anti-inflammatory medication for the two weeks prior to surgery to avoid the risk of bleeding (Tylenol is okay to use). Because the prostate has a rich blood supply, bleeding may occur during surgery.
Long-term risks of radical prostatectomy include incontinence and impotence. With respect to incontinence, approximately one out of five or one out of ten men will develop stress incontinence. This means they may get wet when there is a sudden stress on the bladder such as cough, sneeze, sudden reaching movement, or certain types of physical activity.
What about ED?
With respect to erectile dysfunction, ED, the nerves responsible for erection are immediately adjacent to the prostate. An effort can be made to preserve these nerves with the nerve sparing radical prostatectomy. However, even with nerve sparing, as many as one half of men are unable to achieve an erection after surgery. For those who do regain erection, some report that the erection is less rigid or the quality of the erection is different. For those who do have erection, they have a sense of climax or orgasm, but there is no semen to ejaculate. For those who have difficulty with erection, treatment options are available including Viagra, Cialis or Levitra to help improve erection.
How are men monitored after surgery?
After radical prostatectomy, men are followed at regular intervals with office examination and PSA. In some men, PSA may gradually rise over time in the future, which indicates the potential for disease recurrence. If there is disease recurrence, it is typically because the prostate cancer cells escaped beyond the prostate before it was first removed and does not represent regrowth of the prostate. For men with a rising PSA, subsequent treatment options are available including external beam radiotherapy or hormonal therapy with Lupron injections. These treatments can have additional benefit with respect to prostate cancer management.
Take Home Message
Our practice has performed hundreds of radical prostatectomies over the course of the last 30 years. Many of these patients are quite pleased with their treatment and are willing to share their experience with men recently diagnosed with prostate cancer so that the man with newly diagnosed prostate cancer can receive additional information from the patient’s perspective.
In summary, radical prostatectomy provides an excellent management option for low stage prostate cancer and provides favorable prospects for long-term cure of the disease.
Contact us to request an appointment or ask a question. We're here for you.