
Renal Mass
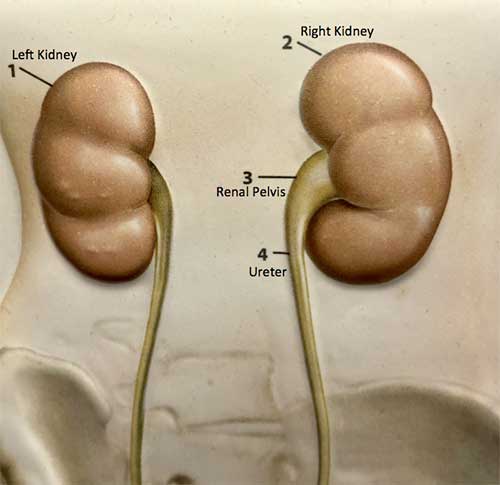
The urinary tract begins with the kidneys, the kidneys, one on each side, sit high in the upper abdomen partially underneath the rib cage.
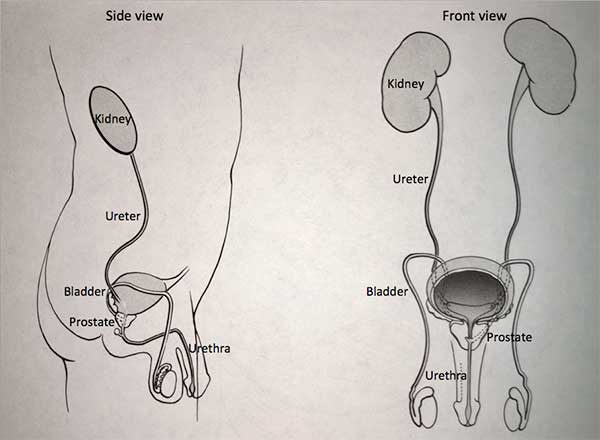
They filter the blood to extract excess waste products and fluid to form the urine. Urine once formed in the kidneys travels through a tube on each side, called the ureter, down to the bladder. Urine is constantly being made by the kidneys and being transported through the ureters into the bladder. The bladder stores urine until full and then empties to the outside through the urethra. The urinary system is the same in both men and women from the level of the kidneys to the bladder. In men, the prostate, which is a gland that is part of the reproductive system, forms the first part of the urethra.
Problems can occur in the kidney which may require surgical removal. These problems can include a renal mass, chronic infection, stone disease or non-function of a kidney.
A renal mass refers to a “growth” in the substance of the kidney. A mass may first be detected because of the presence of flank pain, blood in the urine or an abnormality that can be felt on physical examination. Most often, a renal mass is discovered incidentally during an ultrasound study or a CT scan of the abdomen.
When a renal mass is present, further evaluation depends on its characteristics. Several different types of imaging studies may be carried out in an effort to clarify the nature of the mass. These studies can include ultrasound, CT scan, MRI or a renal nuclear scan. If the studies show a simple cyst, nothing further needs to be done. At least half of people over 40 have simple cysts in their kidney.
If the studies show a complex cyst then the next step may be cyst aspiration. Cyst aspiration is carried out by a radiologist who inserts a needle into the area of abnormality. Fluid within the cyst can then be analyzed. Occasionally a cyst may require surgical exploration to allow direct inspection and possible excision.
If a mass appears solid on the imaging studies, then the next step is typically surgical exploration with plans to remove the mass or the kidney if indicated. 95% of solid renal masses are types of cancers called “renal cell carcinoma.” The optimal treatment for this cancer is surgical removal. Radiation therapy and chemotherapy are not effective. Immunologic therapy, currently under investigation, may provide benefit in some cases. Less than 5% of solid renal masses are benign or non-cancerous types of growth. The distinction between benign and cancerous growths cannot be made with reliability on the preoperative studies.
In general, it is not recommended that a needle biopsy of a solid renal mass be carried out. A needle biopsy may cause severe bleeding. Also, needle biopsy of a renal cell carcinoma may potentially spread the disease, which may then prevent the possibility of a surgical cure. In addition, a biopsy with benign findings (one which does not show evidence of cancer) does not necessarily exclude the possibility of cancer. Solid masses are often mixed tumors that have benign features intermingled with malignant or cancerous features. In these circumstances, a biopsy that does not show cancer does not necessarily indicate the absence of cancer. There are a few select circumstances when a needle biopsy of a solid renal mass may be recommended.
As noted above, nephrectomy, (the surgical removal of a kidney), is done for renal masses, chronic infection, stone disease and poorly functioning kidneys. Open surgery to remove the kidney is usually carried out through an incision that is placed in the midline of the abdomen, under the rib cage or in the flank. Surgery is carried out under general anesthetic and requires several hours. Specific complications related to surgery include bleeding, infection and injury to adjacent organs. General risks of surgery include the possibility of blood clots in either the legs or the lungs, heart difficulties, pneumonia and so forth.
During the postoperative recovery, measures are taken in an effort to minimize these problems. Pneumatic stockings are used to compress the veins in the leg to keep blood flowing. Early ambulation and initiation of calf squeezing exercises are recommended for the same purpose. Patients are encouraged to use an incentive spirometer, a device designed to facilitate taking a deep breath, to prevent the tendency of the lung to “close down” after surgery. Postoperative pain is often managed with the use of patient controlled anesthesia (PCA). PCA provides a set amount of pain medication delivered on a regular basis. The patient can give extra doses as needed. It is programmed so that there cannot be too much pain medicine delivered. A catheter may be placed in the urinary bladder for the first several days to facilitate urinary drainage.
After this surgery, the intestines typically lose their inherent activity for a period of two to four days. During this time period, the bowel is unable to handle any liquids or solid food. For that reason, the patient cannot eat or drink for the first several days. Fluid and nutrition are supplied through the intravenous line. The length of hospitalization typically lasts from 3 to 7 days. Once discharged from the hospital, the patient is allowed to ambulate as much as desired. However, no strenuous activity is allowed for the first six weeks. Follow-up is carried out in the office to monitor the patient’s recovery.
In more recent years, laparoscopy often times with the use of the da Vinci robot has replaced open surgery as the procedure of choice to remove part or the entire kidney. A fiberoptic camera is placed through a “port” (small 1cm incision) into the abdomen. The surgeon can work with operating instruments placed through other “ports” to remove the kidney. A small 3-4” incision in the midline below the belly button is used to remove the kidney. Laparoscopic nephrectomy is less invasive than an open procedure and allows a shorter hospital stay with a quicker return to normal activity.
In many cases the total kidney may not need to be removed, rather a partial nephrectomy may be done in which only the part of the kidney with cancer is removed.
Cancers that occupy only a portion of the kidney can be surgically removed by excising the cancer and a rim of normal tissue using a technique called a partial nephrectomy.
This can be done using open (incision), laparoscopic (keyhole) or robotic surgery. The benefit of a partial nephrectomy is that it allows preservation of healthy kidney tissue. This maximizes overall kidney function and decreases the risk of cardiovascular disease. This is especially important for people with risk factors for impaired kidney function, such as high blood pressure, high cholesterol, diabetes and smoking.
Hazards of partial nephrectomy include bleeding, transfusion, urine leak, infection, damage to surrounding organs (such as bowel or blood vessels), the need for conversion to a radical nephrectomy and anesthetic complications. As with radical nephrectomy, ongoing follow-up to monitor for potential recurrent disease is indicated, which may include a medical history, physical exam, blood work, chest x-ray, and ultrasound or CT scan.
Overall, patients who require nephrectomy do well. For those who require surgery to address a renal mass, particularly one that is discovered in an “incidental” fashion, the long term outlook is usually excellent.
Print PageContact us to request an appointment or ask a question. We're here for you.