
Kidney Stone Overview
How the Urinary System Works
To understand concepts regarding kidney stones, it helps to begin with a description of the urinary system. The urinary tract begins with the kidneys. The kidneys, one on each side, sit high in the upper abdomen partially underneath the ribcage.
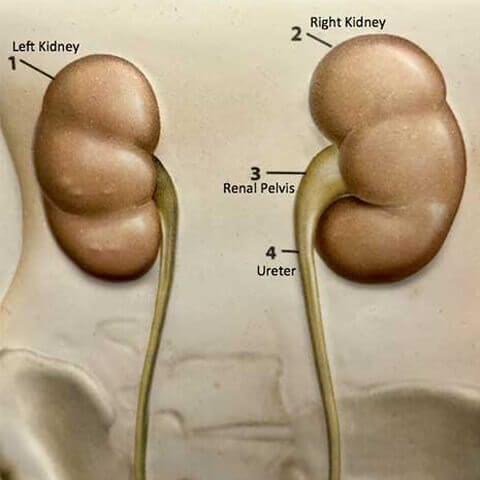
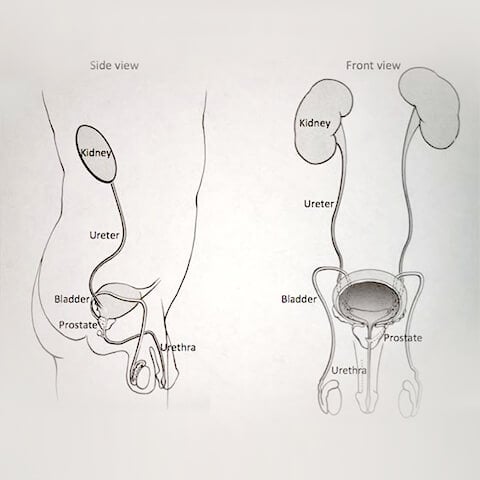
They filter the blood to extract excess waste products and fluid to form the urine. Urine, once formed in the kidneys, enters the first part of the urinary drainage system called the renal pelvis. The renal pelvis funnels the urine into the ureter. Urine travels through the ureter, which is a tube on each side, down to the bladder. Urine is constantly being made by the kidneys, and transported through the renal pelvis and ureters into the bladder. The bladder stores urine until full, and then empties to the outside through the urethra. The urinary system is the same in both men and women from the kidneys to the bladder. In men the urethra is longer and is encircled by the prostate, which is a gland that is part of the reproductive system.
Stones form in the kidney when there is an excess of minerals, usually a combination of calcium, oxalate or uric acid. These minerals begin to crystallize, and then the crystals can join together to form a stone (see Kidney Stone Prevention newsletter for description of stone formation and strategies for stone prevention).
How Stones Are Identified and Why They Cause Pain
Kidney stones may be discovered in different ways. They may present themselves in a dramatic fashion when they cause severe pain, or they may be found incidentally during an imaging study carried out to investigate some other issue. When there is pain suggestive of a stone, an x-ray study is carried out, such as a CT scan and a ultrasound, to determine if a stone is present.
Stones cause trouble when they obstruct the flow of urine from the kidney. Stones can cause obstruction at any point along the pathway from the renal pelvis, through the course of the ureter and down to the junction of the ureter with the bladder. When a stone blocks the ureter, the urine cannot get through. This causes back pressure on the kidney, which then causes the pain. Pain can be severe at times, and may be associated with a reflex nausea and vomiting. The pain can be felt anywhere along the pathway, and may be up in the back or side (referred to as flank pain), or it may extend to the lower abdomen or groin area.
When a stone is present in the ureter, it may obstruct intermittently or an ongoing basis. If a stone blocks the ureter completely, then there is obstruction of the kidney, which can cause severe pain. If the stone rotates slightly (even if it has not moved any further “downstream”), it may no longer block completely, the urine from the kidney can get around the stone, the obstruction may be relieved, the back pressure on the kidney is released, and the pain can subside. Pain may come and go depending on the degree of obstruction.
If a stone is able to make the journey through the ureter and reach the bladder, then the hard work is done, and the stone is typically passed to the outside easily through the urethra. The diameter of the urethra is four times larger than the diameter of the ureter, so typically the stone passes through without difficulty. Many patients urinate the stone to the outside without being aware that they have done so.
Treatment Options for Stones
A variety of treatment options are available for managing stones. When stones are in the kidney, they are often asymptomatic, and in many cases can be left alone. Some stones, particularly small ones, can be present in the kidneys for years, and may never cause trouble. If a stone is causing obstruction the next step depends on the size and location of the stone. When the stone is small enough, it can be approached with a “trial of labor”. The patient tries to pass the stone with increased intake of fluids in an effort to “push” the stone through. Pain pills are made available to help control the pain that can accompany stone passage. When pain begins, it may be helpful to take the pain medication as prescribed, and to get into a tub of hot water or shower for 15-20 minutes. This can provide temporary relief until the pain pills start to work. The patient may also be started on treatment with an alpha blocker (one of the most commonly used is Flomax, also known as tamsulosin). Alpha blockers are medications which are used to dilate the urinary pathway in men with an enlarged prostate, and are also useful to promote dilation of the ureter, which may make it easier to pass a stone.
Intervention for Stones
Intervention for stones may be required for a variety of reasons. The type of intervention again depends on the stone size and location. Reasons to intervene include significant blockage of the kidney, the presence of infection or fever, or the finding of a stone that is too large to pass. One of the most common reasons to proceed with intervention is a failure of the “trial of labor”. If the stone has not passed on its own, or if there have been repeated episodes of pain, then the stone is removed.
Before the 1980’s, intervention for stones required open surgical techniques, which typically required large incisions in the abdominal or flank area, and the need for a hospital stay of a week or more, with another one- to two-month recovery period at home. Fortunately, the current approaches to stone are less invasive.
Intervention for Stones – Stent
When a patient presents with an acute episode of pain and obstruction with a stone, the first step is often placement of a stent. A stent is a thin tube, like a straw, that is placed in the ureter from the kidney to the bladder. It bypasses the obstruction caused by the stone, and allows the kidney to drain. The stent is placed via cystoscopy, a technique done under anesthesia, which does not require an incision or a puncture. The cystoscope, a fiber optic catheter, is placed via the urethra (again, that is the tube that drains urine from the bladder to the outside). A stent can be advanced through the cystoscope from the bladder into the ureter and up into the renal pelvis, which then provides drainage for the obstructed kidney. Stents are very effective at keeping the ureter open, and provide relief of the severe pain caused by obstruction. However, they can cause annoying symptoms for some patients. The end of the stent in the bladder can cause irritation, which may trigger urinary symptoms, including urinary frequency (the sense of the need to go more often), urgency, (the sense of the need to go right away), and pain or discomfort with urination. There may be blood in the urine as well. Some patients experience pain or pressure in the back with urination.
Intervention for Stones – Shock Wave Lithotripsy (ESWL)
The subsequent approach to the stone depends on the size and location. For stones in the upper ureter or the kidney, the next step may be ESWL, also known as shockwave lithotripsy. Carried out with general anesthesia, this technique uses shockwaves that traverse the body to focus on the stone, which then cause fragmentation of the stone into smaller pieces, which can be passed down the ureter.
A variety of outcomes may occur after lithotripsy. In some cases, the stone may fragment into multiple small grains of sand that pass through the ureter without difficulty. In other cases, the stone may break into large fragments, which may pass into the ureter, where they may cause obstruction requiring further procedures for management of stone fragments. Sometimes, a stone may be particularly dense with a very strong crystalline structure, and it may fragment only a little or not at all. In that case, repeat lithotripsy may be required, or a different technique may need to be carried out.
The decision about using a stent in conjunction with lithotripsy may depend on stone size (large stones may do better with a stent to help keep the ureter open while fragments are trying to pass), and the degree of associated obstruction.
After lithotripsy, patients are encouraged to follow the guidelines listed in the Instructions for Passage of Stone newsletter to promote passage of stone fragments.
Intervention for Stones – Ureteroscopy
Another technique used to approach stones is ureteroscopy. In this procedure, also done under anesthesia, a fiber optic instrument is passed through the urethra and the bladder into the ureter to reach the stone. The stone may be entrapped with a basket and removed. Alternatively, if the stone is too large, a laser may be used to fragment the stone into smaller pieces, which can then be removed. Stones in the lower ureter are generally readily accessible with the ureteroscope.
Stones in the upper ureter, or in the renal pelvis, are more difficult to approach with ureteroscopy. As the ureter descends from the kidney to the bladder, it makes a curve.
It can be difficult to reach the upper ureter or renal pelvis due to the curve of the ureter. In some cases, a stent may be placed as a first step. The stent helps dilate and straighten the ureter, which allows more room for subsequent ureteroscopy. The stent is often allowed to remain in place for several weeks, at which time ureteroscopy is more feasible.
After ureteroscopy, a stent may be placed to keep the ureter open. When a stone has been stuck in the ureter, there may often be swelling in the ureter where the stone had been lodged. It may take several days for the swelling to subside. The stent allows the kidney to drain during that period.
It should be noted that with either lithotripsy or ureteroscopy, several procedures may be required to address the stone. Some patients may feel frustrated with the need for multiple procedures that are carried out on a staged basis, but it is helpful to remember that this approach is much better than the open surgical techniques used in the not too distant past.
In any of the circumstances where a stent has been placed, it is necessary to remove the stent. The stent is typically removed via cystoscopy, which is often done in the office, but occasionally be done in the outpatient area with sedation. In some cases when the stent only needs to be in place for a day or two, there may be a string attached to the end of the stent, called a “dangler”, which is allowed to protrude from the urethra. When the time comes for stent removal, the string can be pulled, which removes the stent.
When a patient is troubled with a stone, the doctors use the available techniques available to provide help. However, any intervention carries the potential for hazards to develop as a result of the effort to help. With any of the interventions for stone, there are potential risks, which include the general risks associated with a procedure under anesthesia, such as a heart or lung problem, circulation or blood clot issue, bleeding or infection. In addition to the above, there are potential hazards such as perforation or scarring of part of the urinary system.
In summary, the onset of a kidney stone can be very dramatic. Fortunately, current practice offers the prospects for effective management, and the choice of that management depends on the unique circumstance of each individual patient.
Additional Information
Contact us to request an appointment or ask a question. We're here for you.